 Ελληνικά
Ελληνικά
What do we mean by hematuria?
Hematuria is the existence of red blood cells in the urine in quantities visible microscopically or macroscopically or commonly in this the sick person urinates urine containing blood. Normal urine has a pale yellow color and clear clean appearance. Any change in these characters, usually means the existence of pathological elements (blood, pus, etc.), and therefore a disturbance in the quality of urine. I want to clarify that this is not a disease but a symptom or, as it is called in medical language, a clinical manifestation common to many diseases. Hematuria should be distinguished from urethral bleeding, in which blood comes out of the urethra (the tube i.e. It should be distinguished from urinary bleeding, which is the tube that connects the bladder through which the urine comes out), either continuously or intermittently, but in any case independently of urination.
Usually patients with gross haematuria (where they see blood in the urine), present themselves to the doctor terrified, fearing that they are bleeding excessively, but this does not correspond to reality, since the bleeding is much less severe and hardly anyone needs a transfusion because of hematuria. It is enough to think that when sometimes our nose opens, only 2-3 drops are needed to color a bowl of water. But regardless of the severity of the hematuria, one should never ignore this symptom as it is an indication of a pathological condition until proven otherwise. Of course, there are also the precipitants of hematuria.
But what is the cause or causes of hematuria?
The causes are usually divided into causes that are outside the urinary tract and causes that are in the urinary tract. The causes are different depending on age. Some causes, for example, are usually responsible in a child and others in a 60-year-old adult.
Causes outside the urinary system mainly concern other specialties, but since the urologist is usually the doctor to whom the patient with hematuria is referred and the first to start the diagnostic test, I will mention them briefly.
- • Various hematological diseases such as sickle cell anemia, hemorrhagic tendencies etc.
- • Cardiovascular diseases such as endocarditis etc.
- • Taking anticoagulant drugs
- • Diabetes mellitus, etc.
Here I should note that the possibility that one of these conditions may coexist with a urological condition that causes haematuria should never be excluded. There are also many who argue that certain causes such as taking anticoagulant drugs, bleeding disorders cannot cause haematuria, except if there is some damage to the urinary system such as a neoplasm, inflammation, etc.
As far as urinary causes are concerned, we can easily say that there is no urological or renal condition that cannot cause the appearance of blood in the urine. However, in the search for the causes of haematuria, in us doctors
Are there any characteristics that distinguish hematuria?
Each hematuria usually presents certain characteristics that in many cases can greatly facilitate the diagnosis. We need to see whether the hematuria is initial or final, painful or painful (whether it hurts or not), spontaneous (i.e. without any apparent reason) or after fatigue, travel, etc, small or large, microscopic or macroscopic, so depending on when the bloody urine appears during urination, hematuria is divided into initial if bloody urine comes out at the beginning and then clear towards the end, final if it comes out clear at the beginning and bloody at the end, and total if the urine is bloody throughout the entire duration of urination, from the beginning to the end.
This can easily be ascertained in the doctor's office by the so-called three-glass method, i.e. if the patient urinates in three glasses in succession. Hematuria is classified as initial if blood in the urine is only in the first glass and clear in the others, final if the urine is bloody in the last glass and clear in the others and total if all three glasses have bloody urine. This distinction, although schematic, is of some importance in the search for the origin of hematuria, since the initial hematuria comes mainly from the urethra, the final from the bladder and the total from the kidneys, but this is not absolute, because when the hematuria is large, it presents as total whether it comes from the bladder or the prostate.
Hematuria is also distinguished according to whether it is accompanied by pain, into painless and painful. The former is a frequent manifestation of neoplasms of the urinary tract, while the latter is mainly characterized by lithiasis (a stone in the kidney, ureter or bladder). However, when the hematuria is large enough to form blood clots, one of them may block the ureter and cause colic. Hematuria in neoplasm is also characterized by the fact that it usually occurs automatically without any cause, unlike the hematuria of lithiasis, which most often occurs after fatigue and subsides when the patient lies down.
The severity of a hematuria varies from case to case and, depending on it, the urine is colored, more or less red. In very mild cases, the hematuria is microscopic, while in more severe cases the colour of the urine may be pink, red or give the impression of pure blood. A sign of severe haematuria is the formation of large blood clots - irregularly shaped pieces of blood - which means that there is so much blood that it cannot be diluted in the urine and clots in the urinary tract. These blood clots often take on a shape similar to the part of the drainage pathway from which the bleeding originates. Thus, in heavy renal haematuria, the clots are like spaghetti, i.e. they are exactly the cast of the ureter, while in haematuria originating from the bladder, they are irregularly shaped like "pieces of liver" as they are usually described by the patient.
In contrast to large clots, small clots occur in light haematuria and are usually dark or brownish in colour. The presence of mainly large blood clots often changes the character of a haematuria, which at first may be painless, but becomes painful when one or more clots block the ureter or urethra, causing either colic of the kidney, or severe dysuria and pain in urination, which may reach total retention of urine. Hematocyst usually occurs in large haematuria of the bladder and prostate, and more rarely in bleeding of the kidney, in which colic is more common. Hematocyst often needs immediate surgery if catheterization and washing of the bladder cannot rid it of the clots.
When do we have severe haematuria and how do we distinguish it from light haematuria?
Such large haematuria, which can cause obstruction by haemoptysis, are usually observed in neoplasms of the urinary tract (renal parenchymal carcinoma, renal haemangiomas, papillomas or carcinomas of the renal pelvis and bladder, hypertrophy and more rarely prostate carcinoma, in injuries of the kidney (after a car accident, a fall, an accident in general).) communicating with the drainage fate, after surgery, and sometimes, in polycystic kidneys and in some rare conditions such as the disease of Bournemouth, kidney varices, etc. In the above cases the amount of blood lost is so significant that it can in one or two 24 hours create such a loss of blood that it can force an emergency operation to treat hematuria.
There are some cases when the urine is red, giving us the impression that it contains blood, but this is not due to the presence of blood in the urine, but to some other causes.
Examination of a patient with haematuria
In the examination of a patient with haematuria, attention should be paid to the following points:
The verification whether it is really haematuria or whether the red colour of the urine is due to other causes such as haemoglobinuria, jaundice, porphyrinuria, alkaptonuria, etc. the taking of various drugs such as anti-tuberculosis drugs such as Rifampin, various laxatives very fashionable lately since they are recommended in some diets, some vitamins, etc. The intake of certain foods containing pigments such as beetroot, typical in children after a large consumption of sweets at the weekend, may present red urine on Monday morning (Monday morning disorder as it is typically called), because many foods such as cakes, sweets contain a pigment called rhodamine-b and it colors the urine. Although, in most cases, the appearance of bloody urine is quite characteristic and differs from the appearance of urine containing one of the substances I have mentioned, there are cases of doubtful cases in which only the finding of red blood cells on microscopic examination will confirm the diagnosis of haematuria. But even in this case, it is necessary to examine whether the blood comes from a cause outside the urinary tract, and its mixing with the urine takes place after urination, as in the woman who has her period, where the blood comes from there and during urination it mixes with the urine.
Another point to pay attention to, especially the doctor is: finding the cause of the hematuria. This is based on a very good history and examination and laboratory and radiological testing. The history may mention a condition known to the patient which may involve either the urinary or other system and which may be responsible for the occurrence of haematuria. In the history the patient should describe in detail, if possible, whether this haematuria was painless or painful, whether it hurt, i.e, whether it contained blood clots, blood clots, those little bits we mentioned before, whether it was accompanied by a colic, whether he knows that he has a lithiasis, a stone in some part of the urinary tract, whether the urine was initially red and cleared up towards the end, or whether it was clear at the beginning and became red towards the end, or whether it was red throughout the urination.
Now as far as diagnosis is concerned, an important test is a simple x-ray of the kidneys, ureters and bladder, ultrasound and also pyelography while it is almost always necessary to do a cystoscopy, to look endoscopically with a special instrument the cystoscope directly into the bladder and obviously to take biopsies in an attempt to identify the cause of the hematuria. Here I would like to say that many times the necessary tests can be done and the cause of the hematuria cannot be identified, it is necessary — and especially the doctor must set it — to re-examine the patient after three months, because it is possible that any lesion — and especially a cancer of the urinary tract — which is not apparent with diagnostic tests during this time may develop and give more obvious symptoms, on which the diagnosis will be based, and therefore we should not easily consider as the responsible cause of haematuria, simple conditions such as e.g. We should not easily assume that the cause of the haematuria is usually hidden behind a serious condition.
What does someone need to do if they find out, see blood in their urine or think their urine is bloody?
Surely the first thing he should do is to consult his doctor and even better a specialist doctor, especially a Urologist. He should not be reassured even if his doctor thinks that it is not something serious, he should demand and start a diagnostic test. Treatment of hematuria is directly related to the cause that caused it. Any attempt to treat hematuria as a symptom, ignoring the main condition is not only futile but also dangerous, because in this way the diagnosis of the condition is delayed, which of course when it comes to a urinary malignancy, you understand how dangerous it can be.
If the hematuria is always small when we have gone to our doctor before, we do not need to do anything but as we said the necessary tests should be done to make the diagnosis, while if the hematuria is large and accompanied by clots, blood clots, these pieces we mentioned should be administered a lot of fluids, either orally or by other means to increase diuresis, thus preventing blood clotting and thus flushing the drainage system. At the same time and as long as there is enough blood loss, when someone i.e. He has these signs of severe hematuria for several days then he will most likely need a transfusion.
If the blood clots are too numerous and large to cause difficulty urinating, painful urination or retention of urination, i.e. inability to expel urine, then it will be necessary to insert a catheter and wash the bladder with saline to remove blood cells, and this is most often enough to stop bleeding coming from the bladder or prostate.
As a conclusion, the important thing to keep in mind is that any hematuria small or large, initial or final, painless or painful, can be the only manifestation of a tumor of the urinary system, so the first thing to do is to contact his doctor who will refer him to a specialist in a urologist in this case.
Which urinary tract tumors most commonly cause hematuria?
As I mentioned all urinary tract diseases, and within them all urogenital tumors can potentially cause hematuria, but there are certain malignancies that almost exclusively present with hematuria, such as bladder cancer, while prostate cancer will rarely present with hematuria. So referring to bladder cancer, it must be said that it is the second most common cancer of the urinary tract, while there is a predominance of men over women, reaching 3:1 (2.7:1), more men are affected than women and even the disease is more common in the white race than in the black race. The average age of onset (diagnosis) is 65 years and in almost 85% of those diagnosed with the disease, the cancer is confined within the bladder locally and has not yet gone to the lymph nodes, or distant metastases, this is a very encouraging sign.
Do all bladder tumours have the same prognosis, or does it naturally depend on the stage or some other characteristics?
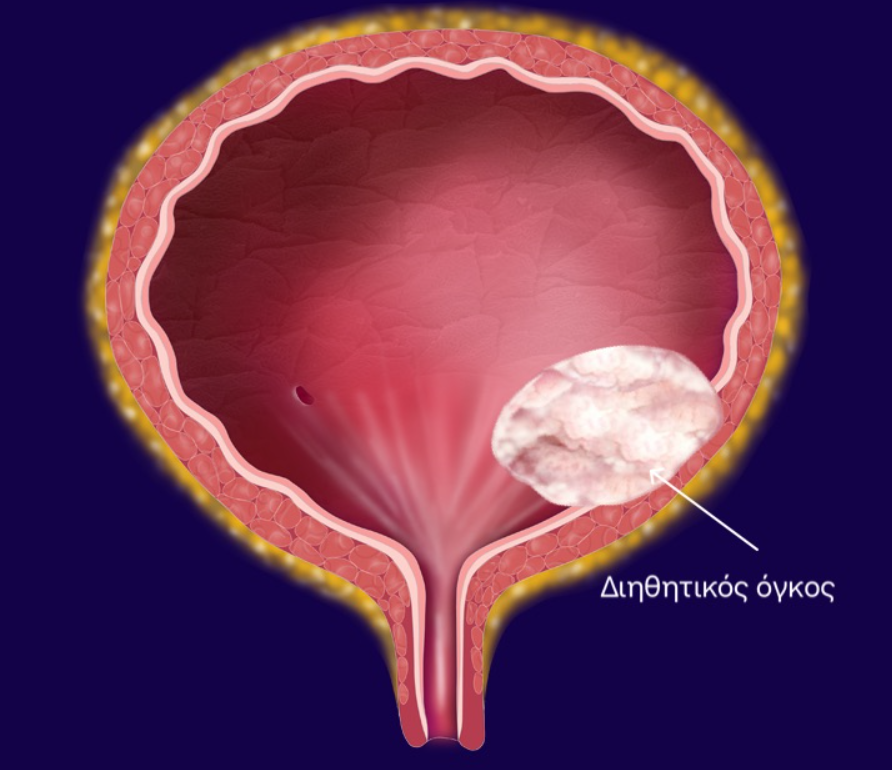
As mentioned earlier 85% of the tumours that present are localised within the bladder and have not metastasised to the lymph nodes or other organs, so bladder tumours are divided into benign which is a very small percentage while malignant tumours are in turn divided into superficial, which have not penetrated the wall of the bladder, the infiltrative ones, those that have reached the wall of the bladder but have not passed through it and finally the metastatic ones which constitute about 15%, and of course have the worst prognosis. This distinction is of great importance, which is why I mention it, for the prognosis and of course for the treatment, i.e. the treatment is different when a tumour is superficial and different when it is invasive or metastatic.
Regarding the manifestation of bladder cancer, we said earlier that it almost always presents with haematuria, which usually has the characters of painless (no pain) total recurrent haematuria i.e. Someone urinates 2-3 times blood does not hurt, reassures and does not consult the doctor with the result after 1 year to reappear hematuria perhaps more severe when the tumor has now grown, so I say again that every hematuria, should be investigated, we should definitely go to the doctor.
Now in other cases besides haematuria the manifestation of the bladder tumour may be a severe frequent urination or difficulty and pain in urination or even recurrent urinary tract infections, recurrent cystitis, indicative of inflammation and infiltration of the bladder wall. In advanced situations one may have more severe symptoms due to infiltration of the entire bladder wall such as residual urine, colic, fever, symptoms that at first sight indicate expansion of the tumor.
As for the diagnosis, of course, which is a medical part, a necessary examination among others is cystoscopy, with which the doctor will see the bladder directly and obviously will take biopsies and will certify the malignancy of the tumor or not.
There is a cure for bladder cancer
Schematically we can say that the treatment is proportional to the nature of the tumor, i.e. superficial tumors (non-muscle invasive bladder cancer) are treated only by transurethral removal, i.e. through the urethra with a special instrument called a cystoscope that has a special knife we remove the tumor as deep as possible and repeat without an incision. Usually these transurethral resections of tumors are accompanied by intravesical injections of drugs through a catheter in the bladder and always of course the outcome and recurrence depends on the stage and nature of the tumor.
Infiltrative tumors (muscle invasive bladder cancer), those that have reached and penetrated the muscle wall of the bladder, usually we treat them with a total, radical cystectomy. What does this mean? Removal of not only the tumor but also the entire bladder, with the obligatory consequence of draining the urine with another technique. Usually we make a new bladder from a piece of intestine that we take and de-tubularize it, i.e. from a tubular shape that has a spherical shape so that it can accept a large amount of urine.
In the deep infiltrating and metastatic tumors that unfortunately have the worst progression and prognosis and we have low success rates, we apply chemotherapy and lately immunotherapy many times in combination or not with radiotherapy.
In most cases, radical cystectomy is a definitive treatment and one can be free forever from this problem i.e. cancer, and this is what we should stay with. It is very important to make an early diagnosis, i.e. before the tumor escapes from the bladder. In conclusion, from all that has been mentioned, the early and early diagnosis of bladder cancer in the early stages and the correct assessment of the stage are of great importance, because the appropriate treatment that will be applied will depend on it and may be definitive.

Early diagnosis — before the tumour escapes from the bladder — is of paramount importance. Hematuria must always be investigated.
Contents
Book an Appointment
Dr. Mertziotis specialises in the diagnosis and treatment of bladder cancer, offering transurethral resection, radical cystectomy and all modern treatment options.
Book an Appointment Online +30 210 6465359