 Ελληνικά
Ελληνικά
What is prostate cancer?
Prostate cancer occurs when abnormal cells grow in the prostate. These abnormal cells can continue to multiply uncontrollably and sometimes spread out of the prostate to nearby or distant parts of the body.
Prostate cancer is generally a slow-growing disease, and most men with a low degree of prostatic cancer aggression live for many years without symptoms and without spreading and becoming life-threatening. However, the disease, in men with a high degree of aggression with prostate cancer spreads quickly and can be fatal. The key is the appropriate treatment option.
What are the symptoms?
In the early stages, there may be no symptoms. In the later stages, some symptoms of prostate cancer may include:
- Frequent urination, i.e., feeling of frequent or urgent urination (sudden need to urinate)
- Dysuria, i.e., difficulty urinating
- Hematuria (presence of blood in the urine) or haemospermia (blood in the semen)
- Pain in the lower back, upper thighs, or hips
These symptoms don't necessarily mean you have prostate cancer, but if you have any of them, visit your doctor.
Which are the risk factors?
Factors most closely associated with increased chances of prostate cancer:
Age
Prostate cancer is an age-dependent disease, which means that the likelihood of developing it increases with age. Specifically, in post-mortem studies the incidence of prostate cancer at the age of less than 30 years is 5%, while this percentage rises to 59% in men over 79 years.
Family history & Genetic mutations
If you have a first-degree male relative with prostate cancer, you are more likely to develop the disease than men who do not have one. The risks are also higher for men whose male relatives were diagnosed when they were young. It has been shown that offspring carrying the BRCA2 oncogene mutation are more likely to develop prostate cancer at a younger age and more aggressive form than those who do not have the BRCA2 gene mutation.
Metabolic syndrome
Patients with increased waist circumference have a higher chance of developing prostate cancer.
Nutrition
There is some evidence that suggest that eating lots of processed meats or foods high in fat may increase the risk of developing prostate cancer.
Lifestyle
There is evidence that suggest that environment and lifestyle can influence the risk of developing prostate cancer.
How is prostate cancer detected and diagnosed?
A doctor will usually do a blood test and/or a clinical exam to check prostate's health.
Blood test (prostate specific antigen (PSA) test)
The result shows if there is an increase in this protein. Depending on the result, further investigation by a specialist may be needed. A high PSA score does not necessarily mean cancer. Prostate's diseases in addition to cancer can also cause an increase in PSA, such as prostatitis.
Digital Rectal Examination (DRE)
Due to the location of the prostate, the doctor who checks the size of the prostate and evaluate abnormalities does so with a digital rectal examination.
Diagnosis
If your tests show that you may have an increased risk for developing prostate cancer, the next step is a prostate biopsy. A biopsy is the only way to make a valid diagnosis of prostate cancer. The most appropriate method is the one that uses multiparametric prostate tomography in combination with transrectal ultrasound with three-dimensional imaging through the perineum — the so-called hybrid biopsies. The urologist takes small tissue samples from your prostate, using very thin, hollow needles guided by ultrasound. A biopsy is usually done as an external procedure. The tissue is sent to a pathologist to determine if the cells are malignant (cancerous) or benign (non-cancerous).
Reducing the risk of developing prostate cancer
Nutrition: Eat nutritious meals. See our Healthy Eating Guide. What is beneficial for the heart is also beneficial for the prostate.
Physical activity / exercise: There is some evidence to suggest that physical activity and regular exercise can be protective factors against cancer. Try to exercise at least 30 minutes of the day.
Hearing a prostate cancer diagnosis from a doctor raises a variety of concerns and questions about what is the best treatment for the disease and how will it affect your future? What impact will the treatment I choose have on my lifestyle? What questions should I ask my doctors? How do I make treatment options for a disease I know so little? Every day, hundreds of people diagnosed with prostate cancer and their families begin searching for answers to these complex questions.
But what does a prostate cancer diagnosis mean?
A cancer diagnosis is a life-changing experience; you need to start making some tough decisions that can have a significant impact on your daily life for many years to come. If you or someone you love has been diagnosed with prostate cancer, you will have several treatment options that are equally effective, but every single one also has its beneficial sides and drawbacks.
Am I undergoing treatment? If so, what treatment?
Focal therapy; Surgery; External radiation; Implantation of radiation spores (brachytherapy); Hormones; Chemotherapy; Or is active surveillance the right choice? In this chapter, we will review the basic material you need to know to make a diagnosis of prostate cancer. We'll talk about PSA (prostate-specific antigen) and the degree of Gleason malignancy, what factors are important in determining outcomes and prognosis, and, in addition, we'll talk about why you should surround yourself with a team of prostate cancer experts, including a wide variety of medical specialties, to help you find the right treatment for you.
Understanding Prostate Cancer Diagnosis
Like many other people diagnosed with prostate cancer, you went to your doctor for a routine exam, and he gave you a PSA and Digital Rectal Exam (through the anus) to detect prostate cancer. Something suspicious comes up, and the doctor sent you for a biopsy. Then, a few days after the biopsy, you were told that prostate cancer was found. Or, you have noticed changes in your urination or sexual function and referred to your doctor. Then, after a complete diagnostic test, including a biopsy, the diagnosis of prostate cancer was made. But what exactly did the doctor examining your biopsy see? Why is it important for you to know what your cancer cells look like? After all, cancer is cancer, right? In fact, the way your cells look under a microscope can tell a lot about your disease. And it will often lead to some very important decisions about treatment options.
Under normal circumstances, your prostate cells, just like all other cells in your body, constantly reproduce and die. And every new prostate cell that grows has the same shape and appearance as all other prostate cells. But cancer cells look different, and the degree to which they look different from normal cells is what determines the degree of cancer. Low-grade cancer cells tend to look very similar to normal cells, while high-grade cancer cells have been altered so much that they barely resemble normal cells.
The Gleason Score
The Gleason score is the system consisting of five distinct patterns that prostate cancer cells tend to transform as they are transformed by normal cells. The scale runs from 1 to 5, where 1 represents cells that are very close to normal, and 5 represents cells that do not resemble prostate cells at all. After examining your biopsy sample under a microscope, the pathologist assigns a Gleason grade to the most common design from 1 to 5, and a second Gleason grade to the next most common design again from 1–5. The two degrees are added, and your Gleason score is determined. In general, the Gleason effect tends to predict the aggressiveness of the disease and how it will behave in your body. The higher the Gleason score, the less the cells behave like normal cells, and the more aggressive the tumor tends to be.

Remember, the Gleason result is not just a simple number. It consists of the two most common Gleason cell designs recognized, and the first number, representing the most common design, is often more important. Thus, although two results may be the same, the individual scores may be different, and therefore the tumor characteristics may be different. For example, a Gleason 7 (3+4) cancer is probably less aggressive than a Gleason 7 (4+3) cancer, even if, technically, both have the same Gleason effect. In some cases, the pathologist may identify a third pattern, which is less common, but this has a higher grade than either of the first two drafts that were involved in the Gleason score. The presence of this third pattern may indicate that the tumor is more aggressive than the Gleason effect of the 2 most common patterns. For example, if a Gleason 4+3 tumor also has some degree of Gleason 5 cells, the cancer would be considered as higher grade overall.
What is the role of PSA?
PSA, or prostate-specific antigen, is a protein produced by the prostate that is released in very small amounts into the bloodstream. When there is a problem with the prostate, such as when a prostate cancer develops and grows, more and more PSA is released, until it reaches a level where it can be easily detected in the blood. PSA plays two different roles in prostate cancer — first as a detection tool before the disease is diagnosed, and then as a way to monitor the progress of the disease once it is diagnosed. In this section, we will focus on the role of PSA as an indicator for disease progression and as a way, if a treatment does its job effectively. Now that you have been diagnosed with prostate cancer, you need to identify these tools that will allow you to have the best possible treatment for your disease.
What does PSA have to do with your Gleason result?
The PSA level you had before you were diagnosed with prostate cancer is often used as an indicator of how advanced your cancer was before it was detected. Usually, the higher the pre-diagnosed PSA, the more aggressive the disease, as well as the Gleason degree. Therefore, this PSA level, combined with your Gleason effect, is used in trying to predict how your tumor will respond to different types of treatment, and how well (in terms of PSA value) you will likely be after initial treatment.
Prognosis of prostate cancer
Despite the efforts of hundreds of prostate cancer researchers, there is no way to predict with certainty exactly how your tumor will behave and how exactly you will respond to any treatment or surgery. Our understanding of how the disease behaves is constantly improving. But, for now, we need to be able to predict what we expect so that we can determine the right treatment for you.
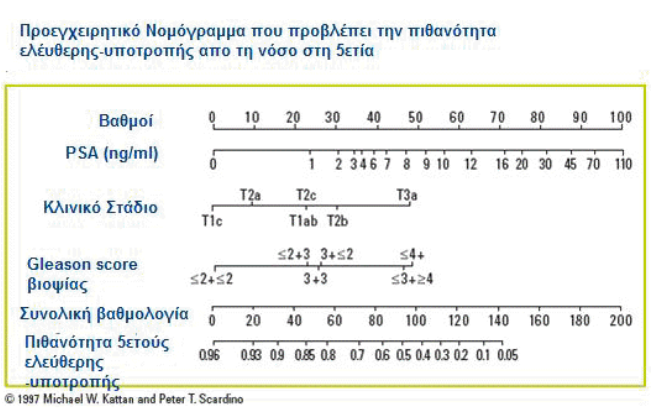
PSA is used both as a disease detection tool and to check its progress once diagnosed. Suppose you want to calculate how likely a particular treatment is to eradicate all your disease. You should consider several factors: The cancer has already metastasized outside the prostate; How aggressive does the disease look (i.e., how much is the Gleason score)? If surgery was performed, was all cancer excluded? Are any of these factors more important than others? Or do they all tell us the same thing? Nomograms are simplified diagrams that have been specifically constructed to calculate each of the necessary contributing factors to provide a single assessment of the likelihood of being disease-free after treatment. The Urologist enters the relevant details of the case, and each factor is assigned a value (grade) depending on how much it has been shown to contribute to the general outcome.
For example, if someone's PSA diagnosis was 2 ng/mL, then he would get 30 points, but if his PSA diagnosis was 30 ng/mL, he would get 80 points. Why? Because, as we noted earlier, a higher PSA diagnosis indicates that the disease has probably spread further, so that this factor will contribute more to its overall outcome. Once all the points for the various factors are added, our nomogram shows the chances that the disease will recur within five years, after the initial treatment. This is referred to as the five-year recidivism rate.
Consider both extremes. If the overall result were 140, the chart would show a five-year probability without relapse of 0.05 or 5%, meaning that 5 people out of every 100 with a score of 140 would be disease-free at five years. At the opposite end of the spectrum, an overall score of 20 would correspond to a five-year probability without disease relapse of 0.93 or 93%, meaning that 93 out of 100 people with an outcome of 20 would have no disease present five years after initial treatment. Knowing how likely it is that you'll be healthy in five years can be reassuring, especially if you're in the 20th grade range. However, if you have any factor indicating that your tumor is aggressive, then you will have a continued risk of recurrence of the disease even beyond five years. It is important to note that laws designed to predict the likelihood of recurrence do not predict death from prostate cancer — a person can live for many years despite recurrences — but they can play an important role in helping decide whether someone should undergo additional treatments or whether they are a candidate to join clinical trials evaluating new treatments.
The role of PSA velocity growth speed
One of the benefits of nomograms is that they allow doctors to consider different factors, including PSA and Gleason grade, which can contribute to successful treatments for you. But what we've found in recent years is that certain factors can help predict outcomes on their own, regardless of any other factor. For example, researchers have looked more closely at how fast PSA increases, or PSA Velocity, and have observed that in some individuals, PSA increases rapidly, while in others, it increases slowly. Having studied the speed of PSA growth in a few hundred people, the researchers found something incredible: people whose PSA increased by more than 2.0 ng/mL per year before undergoing treatment with surgery (radical prostatectomy) or radiation tended to have the worst outcomes overall. They were more likely to have a disease that had already spread, and they were more likely to die from prostate cancer, and even more likely to die from other diseases. This does not mean that people with rapidly rising PSA values will die from prostate cancer, or that their cancers will progress to the advanced stages immediately. It also doesn't mean we should ignore all other factors and only use the speed of PSA elevation to predict prognosis. This simply means that people who fall into this category need to be checked more regularly by their doctors.
Home Prostate Cancer Treatment: Weighing the Pros and Cons of Each Treatment Option
There are three very different types of initial treatments for localized prostate cancer:
- Active surveillance
- Focal therapy
- Surgery
- Radiation therapy
Treatment involving surgery and radiation has in both cases shown positive results as a first-line treatment. Each form of treatment can lead to "definitive cure" — meaning free from the disease for over five years — in more than 90% of people with localized prostate cancer.
Should you start treatment immediately or are you a candidate for careful monitoring or focal therapy? Since we will discuss in this chapter, each of the different therapy options, a careful understanding not only of prostate cancer, but also of how you want to approach treatment is required. Your first step in deciding how to proceed is to understand what each of the treatment options really stands for.
Active prostate cancer surveillance
We know that some prostate cancers grow more slowly than others, and that, some individuals are less likely to get sick and/or die from their cancers. If treatments were easy and had few side effects, unnecessary treatment of slow-growing cancers would adversely outweigh the benefits that proper treatment would bring. As we will discuss in more detail later, the treatments available for prostate cancer are serious, and can have a long-lasting effect on your quality of life. Therefore, deciding when to start treatment can be one of the most difficult decisions. The concept of active monitoring, or watchful waiting, has increasingly emerged in previous years as a viable option for individuals who, for some reason, have decided not to undergo the immediate treatment of surgery or radiation. Although some may say that active surveillance simply postpones treatment, the truth is that for people who have very slow-growing or very early-stage cancers, immediate treatment may not make sense. Instead, they may choose to undergo regular monitoring, with frequent PSA checks, biopsy, MRI and digital rectal examination. In addition, the use of ultrasound, CT and latest PET/CT, bone scintigraphy, or MRI can be used to check the progression of the disease and the need for treatment.
Active surveillance is also a good option for people who have other serious medical conditions that affect their lifestyle, especially if these other conditions are likely to shorten their lifespan. Are you the right candidate for active monitoring? This, of course, can only be determined after extensive discussions with your doctors. Two recent studies evaluating this question have found that individuals who are older than age 65, as well as those who have at the time of diagnosis low-malignancy tumors may benefit with this approach. More clearly, these individuals are likely to have fewer symptoms associated with their disease and are more likely to die with prostate cancer than to die from prostate cancer. Another important factor is for your doctors to consider how healthy you are, i.e., how your general condition is. Many of the treatment options for prostate cancer can be difficult for your body to endure, and the healthier someone starts a treatment, the greater the chances of good results. If you are currently struggling with other diseases, such as heart disease, long-standing high blood pressure, or poorly controlled diabetes, then it is not good to start treatment immediately to avoid its possible complications.
When it comes to making a decision, keep in mind that every person is unique, and there is no magic formula to find out if active monitoring is the right choice for you. If you talk to your doctors and carefully weigh up the pros and cons of different treatment options before making any decision, you need to feel confident that the choice you are making is right for you.
Focal Therapy
In the last 20 years, more and more men are detected in early stages with small tumors occupying 5–10% of the prostate and with a tendency to be in one lobe (European Association of Urology — Guidelines 2019). Also, 1,410 men are required to undergo a PSA test in order to find 48 men with prostate cancer and eventually only 1 of them will die. So the remaining 47 will receive a treatment such as surgical removal of the prostate or radiation with the inevitable consequences of erectile dysfunction (impotence) and urinary incontinence. This is called overdiagnosis and overtreatment. In order to avoid exactly this overtreatment from the other end of active monitoring (which we simply monitor and do not intervene) the need for focal therapy was born.
A course in anatomy and physiology
Before we go into the details of surgery or radiation treatment, you will have to understand where the prostate is, what it is and what surrounds it in the body. Not only it will help you to better understand how each of the different treatments strives to accomplish its goals, it will also help you understand why urological surgeons, oncologists, and radiation therapists have spent so much time perfecting their techniques, toward maximizing the benefit of treatment while minimizing side effects.
The prostate is an organ found only in men. It is a gland that has two basic functions: to help in the proper functioning of the bladder during urination and in normal sexual function by secreting various prostate fluids.
Where is the prostate?
Just below the bladder, in front of the rectum and surrounds (embraces) the urethra, the tube that connects the bladder to the penis through which urine and semen come out. The prostate is the size of a walnut and from the age of 40–50 it begins to grow and swell under the influence of a hormone (the so-called male hormone) testosterone.
Already at the age of 50 half of men have a large (swollen) hypertrophic prostate. At the age of 80 almost the 100%.
Under the prostate, the urethra is embraced by the so-called urethral sphincter. When radical prostatectomy is performed and the prostate is removed, then the bladder and urethra are joined (sutured) to restore its patency. If the sphincter during surgery or radiation is injured or damaged, then some degree of urinary incontinence may occur.
Just behind the prostate are the seminal vesicles, two small glands that secrete about 60% of the substances that sperm consists of. It is estimated that about 10% of people have what is known as seminal vesicle infiltration, meaning that prostate cancer has either been transmitted to or around the seminal vesicles, so the cysts are removed during prostatectomy or become the target during radiation. The loss of prostate and seminal vesicles makes individuals infertile.
Parallel and glued to the sides of the prostate are the vessels and nerves that control the erectile function; If these vessels and nerves are damaged — which was common during prostatectomy until the mid-80s — the ability to achieve an erection is lost. Sexual desire is not affected, but separating or destroying the nerves that control the processes by which erection is achieved leads to erectile dysfunction (impotence). Finally, just behind the prostate and bladder is the rectum, i.e. lower boundary of the intestine just above the sphincter. Solid waste filtered by the body moves slowly into the intestines, and, under normal circumstances, faeces are expelled through the anus after voluntary (deliberate) relaxation of the sphincter. Damage to the rectum caused by radiation, or, more rarely, surgery, can lead to various bowel problems, including bleeding, diarrhea, or the urgent need to bowel movement.
Radical Prostatectomy
The concept of surgical approach to cancer treatment is simple: isolate the tumor and remove it. "Prostate cancer" is actually a misleading term; a better term would be "prostate cancers." Of course, in recent years there has been much debate whether all these small tumors have clinical significance or not. Because usually tumors are of low aggressiveness, they can rarely metastasize and some even consider that they should be considered benign or considered precancerous lesions and do not need treatment but only monitoring. These tumors have a low Gleason score of up to 6 (3+3).
The majority of patients with prostate cancer present the so-called index lesion. It is the site with the largest Gleason score and the largest in size. The theory of index lesion is based on the application of focal therapy. That is, destroying the index lesion focus destroys prostate cancer and does not need to remove the entire prostate. In prostatectomy the entire prostate plus some surrounding tissues are removed, including seminal vesicles. In the most common type of surgery, known as radical retropubic prostatectomy, an incision is made in the lower abdomen and the prostate is cut off behind the pubic bone.
After removing the prostate, the surgeon must suture and join the urethra with the bladder so that urine is able to come out. A catheter inside the bladder is placed for one week to 10 days to allow time for the anastomosis to heal. Another type of surgery, known as radical perineal prostatectomy, is performed less frequently nowadays. Although there is typically less blood loss with this approach, most surgeons find it more difficult to see the surrounding anatomical structures thus the precision needed to maintain erectile function and urinary continence is harder to achieve.
Radical prostatectomy with preservation of neurovascular bundles
Some progress have been made in recent years that are designed to maximize benefits and minimize side effects.
The most important development is the technique of preserving neurovascular bundles. As we mentioned above, the nerves that control erectile function are located exactly parallel to the prostate and in direct contact with it. If the surgeon does not pay any attention to maintaining them, then erectile function is almost always lost. The technique of preserving nerves, originally invented in the 80s, has since been perfected and applied by thousands of surgeons around the world. But that doesn't mean it's always done. The surgeon must carefully remove the prostate at its edges (the capsule) to preserve the nerves. This is an important issue because if there are any cancer cells beyond the place the surgeon has cut off, they can grow and migrate, as a result that you will not have been cured.
If your cancer has already metastasized outside the prostate, the surgeon will have to remove more of the surrounding tissue and therefore he won't probably be able to preserve the nerves. If this is known to you in advance, you will be able to take it into account in deciding your choice of treatment. But sometimes CT or MRI won't show your cancer has metastasized, and the doctor will be forced to make the final decision after he's already started surgery.
In short, the decision on whether to try to preserve the vessels and nerves of erection should be yours — only you know how important it is to maintain your erectile function. But ultimately the decision about preserving the particles is left to the surgeon, his experience, and his clinical judgment. Remember that the goal of surgery is to heal from your illness. If the surgeon does not think he can cure you, leaving the nerves intact, then the nerves will not be preserved.
Nerves are like electrical wires — their function is to carry and transmit a spark to muscle cells by setting them in motion. If the nerve is going to die, the muscle cannot function because it loses the spark of electricity to be able to initiate movement. Theoretically, just as electricians can replace faulty wiring, surgeons should be able to replace faulty nerves. Practically, of course, this is never as simple as it sounds. As we discussed earlier, the nerves that control erectile function run parallel to the prostate. If the surgeon feels, for whatever reason, that nerves cannot be maintained during surgery, erectile function is lost.
Laparoscopic & Robotic prostate cancer surgery
In radical retropubic prostatectomy, a vertical incision is made in the abdomen, below the navel about 10cm in length. The wide opening allows the surgeon to see all internal organs as well as surrounding blood vessels and nerves. But in the 90s, surgeons began to perform laparoscopic prostatectomy with the same surgical technique they used in "simpler" surgeries such as removal of the appendix or gallbladder. In laparoscopic surgery — which is performed by our medical team with great success due to our increased experience — four or five very small incisions (about 1 cm each) are made in the abdomen. Through each incision, the surgeon inserts a narrow and thin instrument with a tiny video camera and/or surgical instruments, which allow the surgeon to visualize and operate on internal structures without opening the entire abdomen.
Further refinements in this technique led to the development of a robotic interface, where the surgeon moves the robot parts, which then control the video camera and surgical instruments inserted into the abdomen very efficiently by performing the operation via remote control. The benefits of laparoscopic surgery are obvious: smaller incisions and less invasive surgical technique lead to less blood loss and the shortest hospital stay. However, because this type of treatment is more challenging than standard "open" surgery, and the learning curve to be effective is steeper, surgical skill becomes even more important.
If laparoscopic surgery is performed by an experienced, competent surgeon, the results can be as good as traditional open surgery, and, in some cases, even better because it is less invasive. The decision whether you should undergo laparoscopic surgery with or without robotic assistance or traditional surgery is yours and only yours.
The importance of surgical dexterity
In every area of life, we recognize that some people are simply better at performing some tasks than others, whether due to experience or natural talent. The same goes for doctors and surgeons. Yes, there are established techniques and standards that any competent surgeon should be able to follow. And there's absolutely no guarantee that even if you were to go to the best surgeon in the world who has performed hundreds of surgeries, you'd get better results than going to someone who has just performed a handful of operations. Radical prostatectomy, like many surgeries, is a very delicate operation, and the difference between a good surgeon and an excellent surgeon can affect the outcome. At the very least, you need to ensure that the surgeon you choose is someone you trust, and someone who has enough experience to not only perform the operation, but also to make a change in treatment after thoroughly documenting and informing you of the change if the need arose.
Prostate Cancer Radiation Treatment
Unlike radical prostatectomy, which uses surgery to eradicate disease from the body, the goal of radiation therapy is to kill prostate cancer cells where they live. To achieve this, very high doses of X-rays target the prostate, focused on small clusters of cancer cells that make up cancer within the prostate gland. The most common type of radiation therapy is external radiation therapy. Oncologists and radiation technicians use CT and MRI to map out the location of tumor cells, and X-rays target those areas.
With three-dimensional conformal radiation therapy, an automated program plots the exact location of prostate tumors so that the highest dose of radiation can reach prostate cancer cells. Because treatment planning with this type of radiation is much more accurate, higher — and more effective — doses can be used with less chance of affecting surrounding tissues. IMRT (Intensity-Modulated Radiation Therapy) takes the dose planning a step further. Studies have clearly shown that releasing higher doses of radiation leads to better results. However, the prostate is located right next to two rather important internal anatomical structures: the bladder and the rectum. Radiation damage to each of these organs can lead to significant urination problems and bowel problems. To avoid these problems, radiation oncologists are tempted to choose to unleash lower doses of radiation — at the expense of reducing the chances of cure. IMRT does exactly what its name says — it allows radiation therapists to modify the intensity of doses and rays to better regulate the radiation released into the prostate while releasing the lowest doses into the cancer cells adjacent to the bladder and anus. With this approach, local side effect rates are further reduced, keeping treatment rates as high as possible.
Regardless of the form of external radiation therapy, radiation therapy sessions usually last five days weekly for about seven or eight weeks and are typically done on an outpatient basis.
The importance of planning doses
Just as surgical ability can play an important role in determining the outcome of prostatectomy, so technical skill and dexterity of the hands can play an important role in determining the effect of radiation. Because the prostate is surrounded by other internal organs, the decision to use a beam of X-rays even a millimeter or two to one side can lead to damage the healthy tissue. The use of computer software helps a lot in planning and targeting doses in prostate tissue, but, in the end, the skill and experience of the radiotherapist will make a big difference. At least, you should seek out a radiation therapist who has extensive experience in a range of irradiation methods and who can objectively help you decide which approach is right for you.
Prostate Cancer Brachytherapy
This form of treatment is generally recommended in localized prostate cancer and like external radiation, this one has high rates of gastrointestinal side effects. The goal of Brachytherapy or implantation of radioactive granules is the same as that of external radiation: to kill prostate cancer cells where they live. The difference, however, is that brachytherapy does it through the prostate itself, while external radiation does it using rays directed at the prostate from the outside.
With this approach, tiny metal granules containing radioactive iodine or palladium, smaller than a grain of rice, are inserted into the prostate through needles from the skin under the testicles. Over the course of several months, the seeds emit radiation into the immediate surrounding area, which kills prostate cancer cells.
By the end of the year, the radioactive material decays — its intensity decreases, and the seeds that remain are harmless. A form of brachytherapy, known as high-dose brachytherapy, does what IMRT does for external radiation: it allows radiotherapists to release very high doses of radiation to very specific areas of the prostate, leaving other areas intact, minimizing side effects.
Other prostate cancer treatments: Focal therapy, Cryotherapy, HIFU & Hormone Therapy
Neoadjuvant hormone therapy: As we will discuss below about hormone therapy, we will see that it is the main treatment in the management of advanced prostate cancer. In the past, a few years ago, researchers had explored ways to incorporate this treatment earlier, in hopes of improving outcomes even further. Hormone therapy is the general term used for any surgical or pharmaco-therapy that prevents the release and/or action of testosterone, the male hormone that nurtures the growth of prostate cancer. Various studies have shown that starting short intervals with hormone therapy can shrink larger tumors, thereby making it easier for radiotherapists to focus on specific areas of the gland, significantly improving outcomes. This use of neoadjuvant hormone therapy is separate and different from the hormone therapy you will receive if your cancer comes back.
Surgery and radiation remain standard treatments for localized prostate cancer, but that doesn't mean other, less popular treatment options aren't right for you.
In the last 20 years, more and more men are being detected at early stages with small tumors that occupy 5–10% of the prostate and tend to be in one lobe (European Urology Association — Guidelines 2019). Additionally, 1,410 men need to undergo a PSA test to identify 48 men with cancer, and ultimately from these, only 1 results in death. Therefore, the remaining 47 will receive treatment with the inevitable consequences of erectile dysfunction (impotence) and urinary incontinence. This is referred to as overdiagnosis and overtreatment. In order to precisely avoid this overtreatment, and from the other end of active surveillance, the need for focal therapy was born.
Cryotherapy (cryosurgery / cryoablation): existed as a treatment option for years, but until a few years ago, it was rarely used. With this therapeutic approach, "needles" are inserted into the prostate through the perineum (the space between the testicles and the anus), so argon in gaseous form or liquid nitrogen enters the prostate, freezing, literally destroying prostate cells and prostate tumors. Over the years, various modifications have been made to avoid damage to neighboring anatomical structures, but rates for erectile dysfunction and incontinence remain high and evidence on long-term effects is limited.
High-intensity focused ultrasound (HIFU) works in exactly the opposite way: prostate cells are heated until they are led to death. A guide is inserted into the rectum, from which very high-intensity ultrasound waves are transferred to the target area. Although this technique remains experimental in the United States, it has been used in Europe for many years with relatively good success rates.
Hormone therapy is a drug treatment designed to suppress the release and/or action of testosterone. Since testosterone is known to fuel the prostate growth of cancer cells, preventing it is a commonly used strategy, in individuals whose cancers are either not cured by topical treatment or are located at a more advanced stage that it makes no sense to perform topical therapy.
The Effect of Prostate Cancer on Men's Daily Life
Prostate cancer affects men's physical and emotional health, relationships, and social life. According to one study, twenty-seven men were subjected to questionnaires at different stages of the disease: nine men before radiotherapy, eight men at 6–8 months after radiotherapy, and 10 men at 12–18 months after radiotherapy. Regardless of the point at which they were interviewed, four areas appeared as important to men: the algorithm of diagnosis, diagnosis, effect of prostate cancer and its treatment on everyday life and living with prostate cancer. Many men didn't understand the consequences of having a high PSA before they had the test. Painful prostate biopsies were considered the worst part of the disease experience. But this has changed with hybrid transperineal biopsies, which are painless. Focal therapy is the new promising treatment that is barely invasive. Radiotherapy was considered less invasive than other treatments, although it is associated with stress and discomfort and of course you have side effects just like surgery.
Focal Therapy: A new promising treatment for prostate cancer
For men with small, localized prostate tumors, focal therapy is offered as an alternative treatment. It concerns a group of carefully selected men with prostate cancer — those who we report as suffering from minimal extent of the disease. The goal of focal therapy is to successfully destroy cancerous foci, while minimizing side effects. Focal therapy is an umbrella term for a variety of non-invasive techniques for destruction of small tumors inside the prostate, while leaving the rest of the gland intact, saving normal prostate tissue.
In appropriate cases, focal therapy can offer many advantages for men with early prostate cancer:
- Focal therapy is performed on an outpatient basis without the need for hospitalization, while in many cases it is performed under local anesthesia or light anesthesia (sedation).
- It can effectively destroy specific cancerous lesions within the prostate, keeping normal prostate tissue and function intact.
- Side effects, including urinary incontinence and sexual dysfunction, may occur less frequently or not at all and may be less severe than those associated with more aggressive treatments such as surgical treatments (robotic radical prostatectomy and open radical prostatectomy).
The application of Focal Therapy
My team and I have been following since 2016 — when for the first time in Greece we started this type of treatment and every year we present our results at international conferences, having now a remarkable experience — a set of strict standards for men who are going to receive focal therapy. This includes a thorough evaluation through multiparametric prostate MRI and hybrid transperineal biopsies, the degree of Gleason malignancy from biopsies, PSA, age, concomitant diseases, etc. to confirm that the tumor is small and localized so that a more extensive treatment such as surgery or radiotherapy is not necessary.
The types of focal therapy we offer to our patients — and only if they meet the criteria for inclusion in our clinical study — are:
- Focal treatment through laser sublimation
- Focal IRE (Electroporation)
- Focal brachytherapy
- Radiofrequency focal therapy
After the end of the focal treatment, our team will closely and carefully monitor the progress of your condition. Except from the prostate specific (PSA) examination and clinical examination, we may recommend you further studies with MRI and ultrasound to evaluate the results of your treatment and you may need to undergo evaluation with the new method of hybrid prostate biopsies.
These studies may also serve as a guide for follow-up biopsy. If follow-up tests show that the cancer is recurring, then we can offer you many other minimally invasive treatment options such as laparoscopic radical prostatectomy, robotic radical prostatectomy and low-dose radiotherapy.
Prostate Biopsy: Combined MRI and ultrasound technique (fusion biopsies)
Prostate adenocarcinoma is often clinically latent, as in many mortuary series it has been detected in up to 80% of men older than or equal to 80 years as well as in about 50% of men older than or equal to 50 years. During the diagnosis and local staging of prostate cancer, from a clinical point of view it is important to distinguish stage T2 (where infiltration does not exceed the limits of the capsule of the gland) from stage T3 (where the tumor has extended beyond the prostatic capsule, to periprostatic fat or adjacent tissues).
The diagnosis of prostate cancer in patients with an elevated prostate specific antigen (PSA) value is mainly based on the results of a biopsy under the guidance of Transrectal Ultrasound (TRUS). Because the accuracy of TRUS in detecting prostate cancer is low, diagnosis is often based on multiple random biopsies, which can lead to false negative results and an increased incidence of complications such as septic infection with fever, hematuria, hemospermia (blood with ejaculation), acute urinary retention (inability to urinate), etc. For these reasons, there was a need to develop an imaging method that allows accurate detection and localization of cancer, guidance of biopsy with TRUS, and taking biopsies not through the bowel but through the skin of the perineum — without passing the needle through the rectum.
This new biopsy method is almost without complications and manages to detect three times more cancers than the conventional biopsy method.
It also manages to show us the suspicious site before we take the biopsy with about 80% accuracy. This means that we do not take blind 12–20 biopsies as with the classical method but only 2–3 according to the suspicious foci. This is achieved by simultaneously using MRI that has discovered possible foci and using these images with special software we convert them into three-dimensional ones where suspicious areas are marked and then placed on the ultrasound — performed by the doctor in real time — and with special sensors guide him to take a biopsy exactly in the area where it should be.
We can accurately estimate the size of the lesion and if then the histological examination proves cancerous, we can easily locate it and treat it even without laser surgery and other minimally invasive methods.
Contents
Book an Appointment
Dr. Mertziotis specialises in prostate cancer diagnosis and treatment, offering robotic radical prostatectomy and all modern treatment options.
Book an Appointment Online +30 210 6465359